‘One Patient at a Time’
Dr. Jim Ledwith ’79 is recognized with the Family Physicians Who Are Changing Our World Award for his leadership in managing opioid treatment and caring for the uninsured
May 8, 2024
By
Mary Beth Bauermann ’24
Editor’s follow-up note: Dr. Jim Ledwith ’79 passed away on July 9, 2024, from complications after a bicycle accident. The W&M Alumni Association will honor him posthumously with the Alumni Civic & Humanitarian Leadership Award on Feb. 8, 2025. His obituary can be found online.
In 2020, seven William & Mary alumni, parents and faculty on the front lines of the opioid crisis were profiled in the W&M Alumni Magazine feature “Hope in Crisis.” Four years later, the crisis is still ongoing and William & Mary alumni are still fighting it. One such alumnus is Dr. Jim Ledwith ’79, a retired family physician, opioid management consultant and learning community mentor at UMass Memorial Health.
Ledwith received the Family Medicine Education Consortium (FMEC) 2023 Family Physicians Who Are Changing Our World Award last fall for his “service and advocacy for responsible care for patients who depend on opioid medication” as well as his leadership in caring for the uninsured. The award additionally acknowledges Ledwith’s leadership in training family physicians on how to treat pain and opioid use disorder.
“Dr. Ledwith has defined his career through service to vulnerable patient populations,” Dr. M. Diane McKee, professor and chair of the UMass Chan Medical School’s Department of Family Medicine and Community Health, wrote in nominating him for the award. McKee also cited Ledwith’s consistent mentorship of students, physicians and junior faculty members.
“I feel so fortunate to work alongside a physician-humanist of his caliber,” she wrote.
In recognition of his modeling of compassionate care, Ledwith was inducted into the Gold Humanism Honor Society by election of the medical student membership, according to the award nomination.
Ledwith says he is honored to receive the award, noting, “I’ve collaborated on many efforts with the FMEC over my years of teaching since I’ve been at UMass, working with a group that discussed how to safely prescribe opioids and how to treat opioid use disorder in family medicine residencies. I felt good about the work I did with them, and it’s been special to be recognized by them.”
Since retiring from his primary care practice, he continues to work as a physician consultant at the Massachusetts Consultation Service for Treatment of Addiction and Pain, training and guiding his fellow physicians in compassionate care for patients dealing with complex pain and addiction conditions.
A Medical Mission
 Ledwith didn’t start his career intending to focus on opioid use disorder. Originally from New Jersey, he followed in his father’s footsteps by attending college in Virginia and majoring in chemistry, a decision influenced by his own early passion for science and math. Noting that his father and older brother both went to Virginia Tech, and his older sister attended the University of Virginia, Ledwith says, “I was smarter — I went to William & Mary.” His younger brother and sister, Brian Ledwith ’81 and Jennifer Ledwith Gerkin ’84, followed him to W&M.
Ledwith didn’t start his career intending to focus on opioid use disorder. Originally from New Jersey, he followed in his father’s footsteps by attending college in Virginia and majoring in chemistry, a decision influenced by his own early passion for science and math. Noting that his father and older brother both went to Virginia Tech, and his older sister attended the University of Virginia, Ledwith says, “I was smarter — I went to William & Mary.” His younger brother and sister, Brian Ledwith ’81 and Jennifer Ledwith Gerkin ’84, followed him to W&M.
After graduation, Ledwith enrolled at the Medical College of Virginia (now Virginia Commonwealth University School of Medicine). His older sister, a family physician, influenced him to sit in on family medicine and primary care rounds whenever he could.
“I found out I could really have a very diverse career,” he says. “I chose family medicine as opposed to limiting myself to one body part — that never had an appeal to me.”
Ledwith’s work with opioid use disorder and uninsured patients started in Tappahannock, Virginia, a rural community in which roughly 25% of his patients lacked insurance to pay for medical care.
“I was doing a fair bit of free care within my own practice,” he remembers. “Eventually, I was able to find volunteers who assisted me in developing a free clinic, which we initially called Tappahannock Free Clinic. This provided an evening a week of free care for folks who lacked insurance.” The clinic is still operating today as the Ledwith-Lewis Free Clinic.
Ledwith has many stories from his time in Tappahannock working with patients dealing with addiction. He tells about a young man who developed an addiction to prescription pain pills and heroin: “From our little town of Tappahannock back in the 1990s, he had to drive into the city of Richmond — over an hour away — to get to the clinic to get his dose of Methadone treatment in the morning and then go to work,” Ledwith says. “He could not get to work on time after getting that morning dose repeatedly, so he would wean himself off, then relapse and then realize he needed help, so he would go back to the clinic. He went through that process of weaning off the Methadone three times but after the third time, he overdosed on heroin and had a permanent brain injury. His children, who are now young adults, can only see their dad in a nursing facility at this point. That was tragic.”
Battling an Epidemic
Although Ledwith left Tappahannock in 2005 after 19 years to care for his aging parents in Massachusetts, his work with the uninsured continued. He provided care and served as faculty advisor for the UMass Chan Medical School’s student-run free health care programs. He also practiced family medicine in the small city in the throes of a heroin epidemic. “We were seeing at least one person a week suffer an overdose or major complications of their drug abuse,” he recalls.
Figures from the Centers for Disease Control and Prevention indicate a steep increase in opioid-related overdose deaths since that time, from fewer than 20,000 nationally in 2005 to more than 80,000 in 2021.
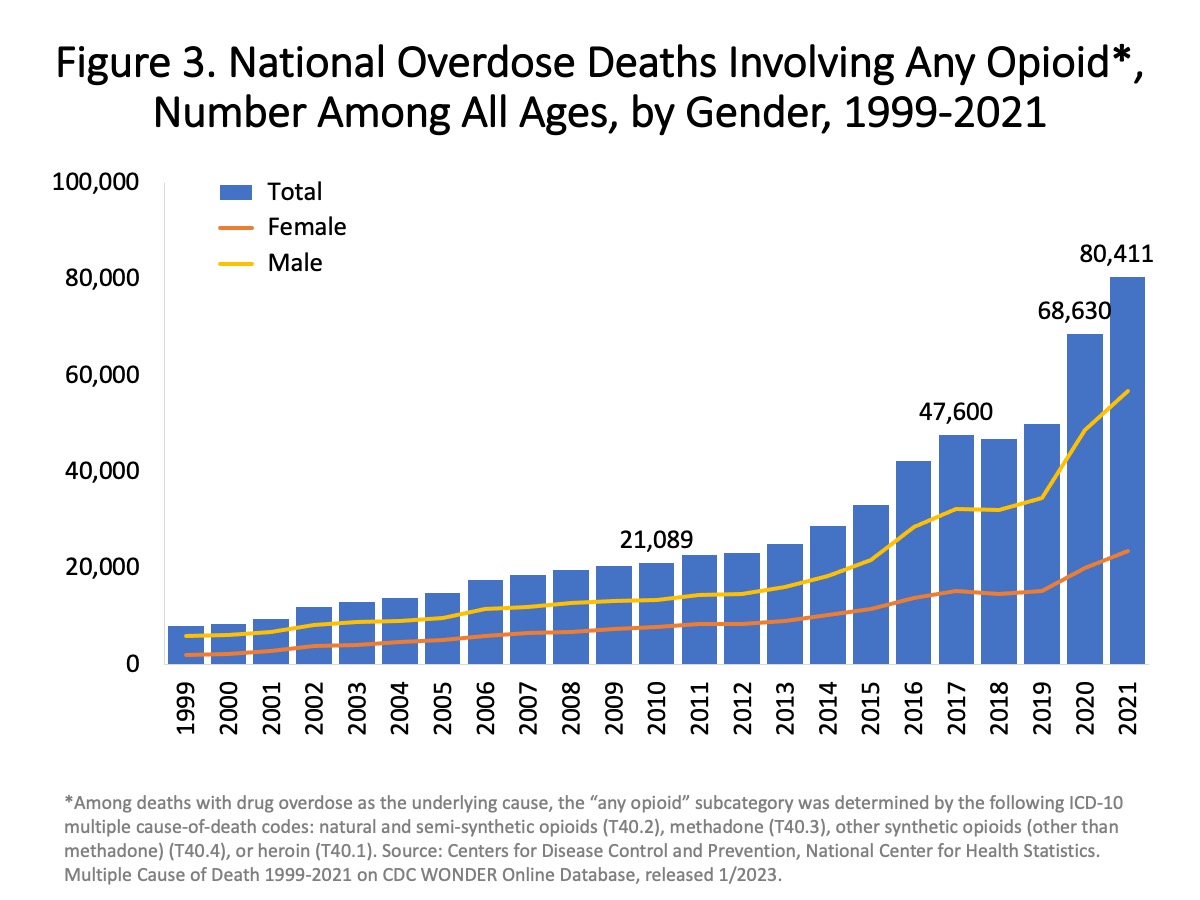{kind=link}
In 2001, a new medication emerged to treat opioid abuse disorder, which Ledwith adopted: buprenorphine/naxalone, known as the brand Suboxone. Buprenorphine can be obtained from any licensed prescriber, making it accessible without traveling to methadone treatment programs. The limiting factor, Ledwith says, has been the willingness of physicians, nurse practitioners, and physician assistants to provide this lifesaving therapy. He expects access to improve since the 2001 federal requirement for eight hours of special training was withdrawn in 2022.
In addition to greater access to the buprenorphine treatment, Ledwith observed dramatic changes in his patients, who started being able to take care of themselves, show up for work and focus on employment.
“It redefined conversations from, ‘Why are you abusing heroin?’ to ‘It sounds like there’s a problem with the way you’re using this medicine and there’s a way to treat it,’” he says.
Upon seeing his patients’ transformations, Ledwith’s family medicine residents were eager to learn how to provide the treatment. “This led to me being highly involved with developing a curriculum for our trainees and then spreading that to other residency programs throughout the Northeast and even across the country,” he says.
Although he retired from his primary care practice at UMass in 2023, Ledwith has continued his involvement with UMass Memorial Health’s Opioid Crisis Task Force, aka “Team Opioid.” In this role, Ledwith reviews clinical practice guidelines and the tools available for hospital and community physicians to assure safer prescription management. The team previously revised and implemented a trackable, user-friendly patient agreement about the purpose of the prescribed drug, how it should be taken and how a doctor would prescribe and monitor it. They are now helping clinical teams use the system tools to assure that prescribing is safely managed. “We’re documenting this for everybody on a long-term opioid and committing to review it with patients on a yearly basis,” he says.
Ledwith acknowledges that caring for patients with opioid use disorder can be daunting for primary care physicians, who are often overworked. He emphasizes the importance of regularly reviewing reports that track safe monitoring practices to decrease the burden on doctors. This practice, he says, can be managed by a medical assistant or an office coordinator, who can review reports and identify who is overdue for an office visit or needs a drug screening test the next time they come in.
“We’re recommending that everybody on chronic opioids have a screening test — at least twice per year — for drugs of abuse and to confirm that they’re actually taking the drug that’s being prescribed,” he says. Ledwith routinely carries nasal naloxone, aka “Narcan,” to have it available in the event of an accidental overdose, and he recommends physicians co-prescribe it. “When they have a system in place for safely managing prescriptions, it actually becomes a pleasurable experience for doctors instead of something to dread.”
His goal for the future is to “develop approaches of creating new bridge clinics that will do the work of improving the chronic opioid prescribing for pain as well as getting people struggling with pain killers stabilized on Suboxone.” He says that when the patient is stable, “it’s easier for the primary care physician to continue the therapy that seems to be working.”
Ledwith enjoys his remote consulting work in retirement.
“It's been very fulfilling, and I have loved being a teacher and mentor to medical students and resident physicians,” he says. “Working with my colleagues who are in practice is equally fulfilling in terms of being able to address a very keen practice need and guide people in how to implement systems that allow them to more comfortably take care of patients with a complex problem. I’ll try to continue doing so as long as I can.”
He notes that while final statistics are still pending, early data suggests that the U.S. may finally be at a point where we have not had another increase in opioid overdose deaths in 2023, compared to previous years.
“I'm not sure I changed the world a lot,” he says, “but I guess I’m changing it a little bit at a time. One family doctor and one patient at a time.”